 Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
The meniscus is a C-shaped piece of tough, rubbery cartilage like structures that acts as a shock absorber between your shinbone and your thighbone. It can be torn if you suddenly twist your knee while bearing weight on it.
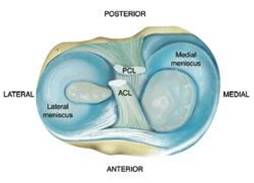

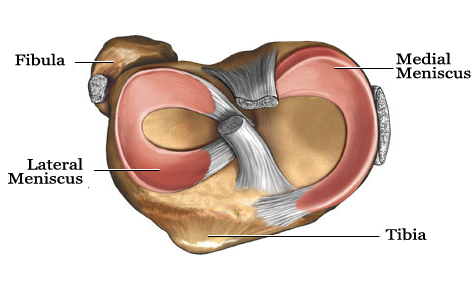
Each knee joint contains an inner and outer meniscus (medial and lateral meniscus). They become thinner towards the middle of the joint. The meniscal cartilages sit on top of, and are in addition to, the usual thin layer of cartilage which covers the top of the tibia. The menisci act like shock absorbers to absorb the impact of the upper leg on the lower leg. They also help to improve smooth movement and stability of the knee.
When people talk about a cartilage injury to a knee, they usually mean an injury to one of the menisci. However, the knee also has cartilage covering the ends of the bones in the joint – this is called articular cartilage – and damage can occur here as well. The areas of articular cartilage can be seen in the side view of the knee joint in the diagram.

https://www.youtube.com/watch?v=9umiq0g50VQ&feature=youtu.be
Meniscal cartilage injuries
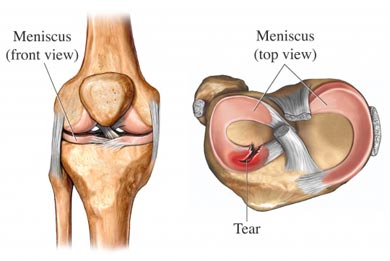
The knee is commonly injured in sports, especially football, volleyball and badminton. You may tear a meniscus by a forceful knee movement whilst you are weight bearing on the same leg. The classical injury is for a footballer to twist (rotate) the knee whilst the foot is still on the ground – for example, whilst dribbling round a defender. Another example is a tennis player who twists to hit a ball hard, but with the foot remaining in the same position. The meniscus may tear fully or partially. How serious the injury is depends on how much is torn and the exact site of the tear.
Meniscal tears may also occur without a sudden severe injury. In some cases a tear develops due to repeated small injuries to the cartilage or to wear and tear (degeneration) of the meniscal cartilage in older people. In severe injuries, other parts of the knee may also be damaged in addition to a meniscal tear. For example, you may also sprain or tear a ligament.
Meniscal cartilage does not heal very well once it is torn. This is mainly because it does not have a good blood supply. The outer edge of each meniscus has some blood vessels, but the area in the centre has no direct blood supply. This means that although some small outer tears may heal in time, larger tears, or a tear in the middle, tend not to heal.

What are the symptoms of a meniscal tear?

The symptoms of a meniscal injury depend on the type and position of the meniscal tear. Many people have meniscal tears without any knee symptoms, especially if they are due to wear and tear (degeneration).
- Pain. The pain is often worse when you straighten the leg. If the pain is mild, you may be able to continue to walk. You may have severe pain if a torn fragment of meniscus catches between the tibia and femur. Sometimes, an injury that you had in the past causes pain months or years later, particularly if you injure the knee again.
- Swelling. The knee often swells within a day or two of the injury. Many people notice that their knee is slightly swollen for several months if the tear is due to degeneration.
- Knee function. You may be unable to straighten the knee fully. In severe cases you may not be able to walk without a lot of pain. The knee may lock from time to time if the torn fragment interferes with normal knee movement. Some people notice a clicking or catching feeling when they walk. (A locked knee means that it gets stuck when you bend it and you can’t straighten it without moving the leg with your hands.)
Note: a ‘clicking’ joint (especially without pain) does not usually mean you have a meniscal tear.
For some people, the symptoms of meniscal injury go away on their own after a few weeks. However, for most people the symptoms persist long-term, or flare up from time to time, until the tear is treated.


How is a meniscal tear diagnosed?
- The story and symptoms often suggest a meniscal tear. A doctor will examine the knee. Certain features of the examination may point towards a meniscal tear.
- Your doctor may sometimes advise an X-ray of the knee – but this is often not necessary. An X-ray will not show cartilage tissue, but it can check for any bone damage which might have also occurred with the injury.
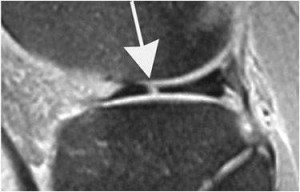
- The diagnosis can be confirmed by an MRI scan of the knee or by arthroscopy (keyhole surgery)




What is the treatment for a meniscal tear?
When you first injure your knee the initial treatment should follow the simple PRICE method:
- Protect from further injury.
- Rest (crutches for the initial 24-48 hours).
- Ice (apply ice (wrapped in a towel, for example) to the injured area for 20 minutes of each waking hour during the first 48 hours after the injury).
- Compression (with a bandage, and use a knee brace or splint if necessary).
- Elevation (above the level of the heart).
These actions, combined with painkillers, help to settle the initial pain and swelling. Further treatment will then depend on:
- The size of the tear.
- The severity of symptoms.
- How any persisting symptoms are affecting your life.
- Your age.
- Your general health.
Non-operative treatment
Small tears may heal by themselves in time, usually over about six weeks. Some tears which do not heal do not cause long-term symptoms once the initial pain and swelling subside, or cause only intermittent or mild symptoms. In these cases, surgery may not be needed. You may be advised to have physiotherapy to strengthen the supporting structures of the knee, such as the quadriceps and hamstring muscles.
Surgery
If the tear causes persistent troublesome symptoms then an operation may be advised – although evidence for the benefit of some types of surgery is variable. Most operations are done by arthroscopy (see below). The types of operations which may be considered include the following:
- The torn meniscus may be able to be repaired and stitched back into place. However, in many cases this is not possible.
- In some cases where repair is not possible, a small portion of the meniscus may be trimmed or cut out to even up the surface.
- Sometimes, the entire meniscus is removed.
- Meniscal transplants have recently been introduced. The missing meniscal cartilage is replaced with donor tissue, which is screened and sterilised much in the same way as for other donor tissues such as for kidney transplants.

Arthroscopy
This is a procedure to look inside a joint by using an arthroscope. An arthroscope is like a thin telescope of 4.5mm diameter with a light source. It is used to light up and magnify the structures inside a joint which can be seen on an high definition television monitor. Two or three small (less than 1 cm) cuts are made at the front of the knee. The knee joint is filled up with fluid and the arthroscope is introduced into the knee. Probes and specially designed tiny tools and instruments can then be introduced into the knee through the other small cuts. These instruments are used to cut, trim, take samples (biopsies), grab, etc, inside the joint. Arthroscopy can be used to diagnose and also to treat meniscal tears.
- Meniscectomy. In this procedure, the damaged meniscal tissue is trimmed away when it is moving inside the knee joint after being torn from its peripheral attachement.
- Meniscus repair. Some meniscal tears can be repaired by suturing (stitching) the torn pieces together. Whether a tear can be successfully treated with repair depends upon the type of tear, site of tear as well as the overall condition of the injured meniscus. Tears in the outer zone are usually selected for repair . The blood supply in the inner zones of the meniscus is very little and chances for healing are less in this area.


Because the meniscus must heal back together, recovery time for a repair is much longer than from a meniscectomy.
Following surgery, you will have physiotherapy to keep the knee joint active (which encourages healing) and to strengthen up the surrounding muscles to give support and strength to the knee.
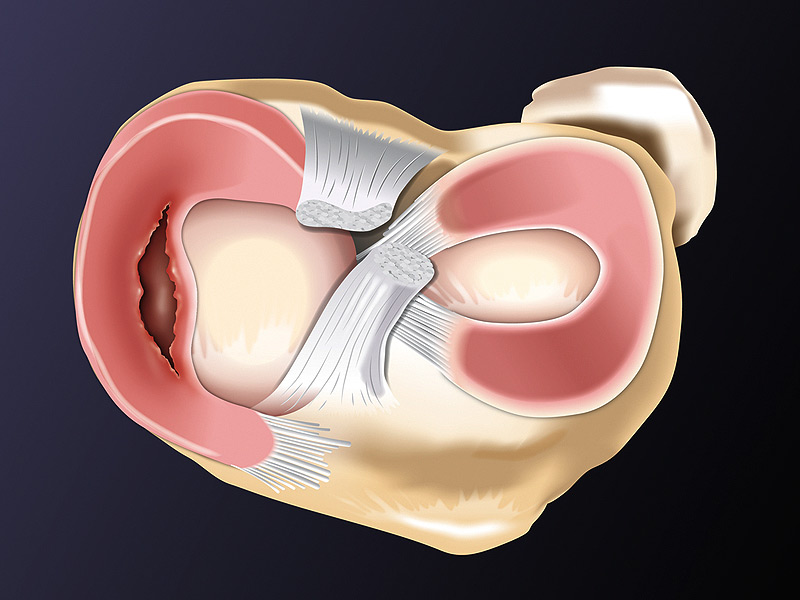
Flipped Meniscus tear
A meniscus tear is like a stone caught inside a ball bearing — every movement grinds, wears, and damages the joint. Repairing or replacing the meniscus removes that ‘stone’ so the knee can glide smoothly again



Partial Meniscectomy

Meniscus allograft transplantation
When the meniscus can’t be saved, the next step is restoring what’s lost — explore Meniscus Allograft Transplant and get your knee back to life.
Meniscus allograft transplant is a procedure where a donor meniscus is used to replace a severely damaged or absent meniscus.
It helps restore shock absorption, protect knee cartilage, and reduce pain in young, active patients.
This surgery is typically advised when previous meniscus repairs or partial meniscectomies no longer provide relief.
With modern arthroscopic techniques, recovery is smoother and aims to preserve long-term knee function and joint health.

Physiotherapy and Rehabilitation after Meniscus balancing
After surgery we may need to put your knee in a brace to keep it from moving. If you have had a meniscus repair procedure, you will need to use crutches for about a month to keep weight off of your knee.
Once the initial healing is complete, you will be prescribed rehabilitation exercises. Regular exercise to restore your knee mobility and strength is necessary. You will start with exercises to improve your range of motion. Strengthening exercises will gradually be added to your rehabilitation plan.
For the most part, rehabilitation can be carried out at home, although your doctor may recommend physical therapy. Rehabilitation time for a meniscus repair is about 3 months. A meniscectomy requires less time for healing — approximately 3 to 4 weeks.
Repair of Bucket handle tear of Meniscus
Arthroscopic Latarjet changes life of Violinist

Recent Posts

Sr. Consultant Orthopedic Surgeon, Prof & Head,
Institute of Advanced Orthopedics, MOSC Medical College Hospital, Kolenchery, Kochi, Kerala, India - 682311




