 Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
What is a dislocated shoulder?
This means your shoulder has come out of joint. This can be very painful and sometimes
can put pressure on the nerves and blood vessels of the arm.

Shoulder dislocation
The shoulder is a ball and socket joint. However, whereas the hip has a deep socket, the shoulder socket is more shallow. This gives the shoulder a greater range of movement than the hip but, in return, it is more unstable.
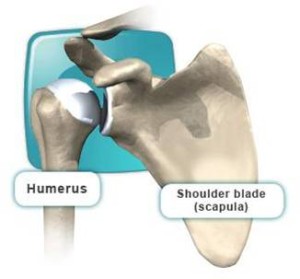
The articulation of the shoulder joint is between the head of the humerus and the shallow glenoid cavity of the scapula. The glenoid cavity is deepened by the glenoid labrum (a fibrocartilaginous rim). The shoulder joint is stabilised by the shoulder labrum and capsule (as well as the surrounding muscles)

Anatomy of the shoulder joint
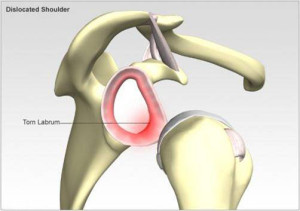
The labrum is a cartilage-like ring surrounding the glenoid (see below).
The capsule is a series of ligaments that connects the humerus to the glenoid.
When the labrum and/or ligaments stretch or tear, the shoulder has a greater tendency to dislocate. This is known as instability, which can lead to greater and more painful shoulder conditions, especially dislocation and subluxation.
Dislocation and subluxation are the telltale signs of instability .

The socket is often compared to a golf tee and the ball to a golf ball. If a certain amount of the “tee” is damaged, it can no longer hold the “ball”. This is when a bony procedure to fix the “tee” may be necessary.
Presentation
The Shoulder joint is one of the most commonly dislocated joints.
Dislocated shoulders tend to occur more often in males than in females. This is probably because of association with contact sports.
In men, the peak age is 20-30 years and in women it is 61-80 years (due to susceptibility to falls).
The common presentation are:
- Pain caused by shoulder injury
- Repeated shoulder dislocation
- Repeated instances of the shoulder giving out
- A persistent sensation of the shoulder feeling loose, slipping in and out of the joint, or just “hanging there”
Repeated episodes of dislocation should raise the possibility of hypermobility or Ehlers-Danlos syndrome being present.


There is usually a history of fall or sudden twist of the arm with pain in the shoulder and inability to move it.
Anterior dislocation
- The patient with anterior dislocation holds the arm at the side of body in external rotation. There will be inability to lift the arm up.
- The shoulder loses its usual roundness. An anterior bulge may be seen in thinner patients. The humeral head may be felt in front of the shoulder.

Posterior dislocation
- Posterior dislocation is much less obvious on examination and can easily be missed. Patients may sometimes present with a long-standing posterior dislocation.
- The arm will be will be at the side of the body and rotated inwards.
Investigations
A Skiagram or Xray will show the mal-aligned bones if taken in the dislocated position before correction. But after a closed reduction the xray will look normal. But there will be soft-tissue tears of the labrum and capsular ligaments which can be visualized only in MRI (Magnetic resonance Imaging)
If the Shoulder joint dislocated more than one time, the bones forming the joint will show signs of erosion of the parts which rub each other while dislocating. The erosion on the upper lateral surface of the Head of humerus is called a Hill-Sach’s lesion. The bone defect on the inferior part of the glenoid or the shoulder cup is called the Bony Bankart lesion.

MRI Scan


Treatment
Dr. Sujit Jos commonly attempts to address multidirectional and some unidirectional shoulder instability without bone loss with conservative measures. Non-operative measures include anti-inflammatory medications (NSAIDs), activity modification and a physical therapy program to strengthen the muscles that surround the shoulder to provide dynamic stabilization of the joint.
Physiotherapy – to train the shoulder muscles to control the shoulder correctly and prevent further instability
Surgery – A number of procedures are available to remedy chronic instability, depending on the causes and findings on investigations.
Types of Surgery:
- Arthroscopic Procedures – through keyhole surgery.
- Open Shoulder Procedures – depending on the problems found, such as the Latarjet procedure for glenoid bone loss or open capsular repair for HAGL lesions.
Prevention
Strong shoulder muscles remain the best defence against shoulder dislocation, subluxation, and, thus, instability. Exercises that build up these muscles around the shoulder should be done. The key is to balance the muscles around the shoulder and ensure not only the ‘mirror’ muscles are exercises (those that you can see when looking in the mirror). Good core stability and posture are also important.
Adequate warm-up before activity and avoidance of high-contact sports will help prevent instability-causing injuries.
Complications of anterior dislocation
- Axillary nerve damage.
- Brachial plexus, radial and other nerve damage.
- Axillary artery damage (more likely if brachial plexus injury is present – look for axillary haematoma, a cool limb and absent or reduced pulses).
- Associated fracture (30% of cases) – eg, humeral head, greater tuberosity, clavicle, acromion.
- Recurrent shoulder dislocation.
- Anatomical lesions:Bankart’s lesion: avulsion of the antero-inferior glenoid labrum at its attachment to the antero-inferior glenohumeral ligament complex.[10] There is rupture of the joint capsule and inferior glenohumeral ligament injury.
- Hill-Sachs lesion: a posterolateral humeral head indentation fracture can occur as the soft base of the humeral head impacts against the relatively hard anterior glenoid. Occurs in 35-40% of anterior dislocations and up to 80% of recurrent dislocations.
- Rotator cuff injury.
First aid management
An anterior shoulder dislocation cannot be effectively immobilised with a simple sling, as the arm is locked in a degree of abduction and cannot be brought comfortably against the chest wall.

- The shoulder and arm should be splinted in the abducted position in which they are found.
- A pillow or rolled blanket can be placed in the space between the arm and chest wall for comfort and support.
- The elbow should be flexed to 90° and a sling applied to support the arm.
- The pillow and sling can be secured as a unit to the chest.
Recurrent dislocation
- Dislocation of the shoulder is often associated with damage to the joint capsule (as in Bankart’s and Hill-Sachs lesions) and this can lead to instability and predispose to recurrent dislocation.
- 80-94% of patients who have a dislocation under the age of 20 years will have a recurrence of their dislocation.
- 26-48% of those younger than 40 years will have a recurrence.
- 0-10% of those older than 40 years will have a recurrence.
- A single dislocation in a young man who plays contact sport may well merit referral to an orthopaedic surgeon to assess stability of the joint with a view to a stabilisation operation. Two dislocations in a young person certainly merit Arthroscopic Bankart surgery.
- There are several stabilisation procedures, dependent upon the nature of the lesion.
Arthroscopic Bankart Procedure
(Keyhole surgery of shoulder dislocation)
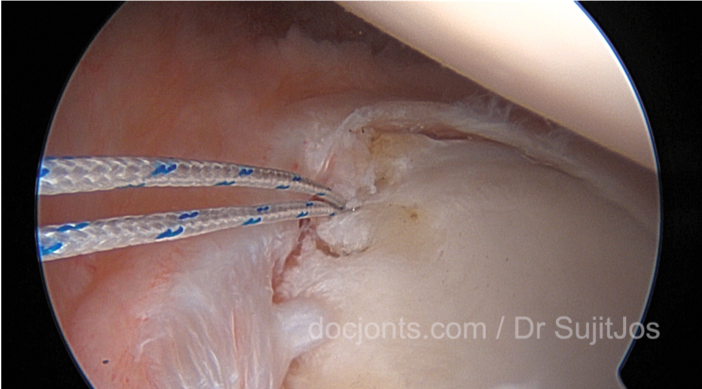
The operation involves reattachment and tightening of the torn labrum and ligaments of the shoulder (see pictures below). This usually done using sutures and small bone anchors.
The glenohumeral joint provides 60% of shoulder motion. It is a modified ‘ball and socket joint’. The humeral head moves in a complex manner over the glenoid with a combination of rolling, gliding and sliding actions.

The labrum is wedge-shaped and attaches almost completely around the edge of the glenoid. This creates a deeper cup for the glenoid socket. This is important because the glenoid socket is so flat and shallow that the ball of the humerus does not fit tightly. The labrum creates a deeper cup for ball of the humerus to fit into. This makes a contribution to the stability of the joint.
The labrum may become detached in patients with dislocations of the shoulder (causing a Bankart lesion ).


An arthroscope is inserted through a small skin incision from the back of the shoulder and special instruments are inserted through portals (green) through the front of the shoulder. The surgeon operates looking at the magnified image on an television monitor.


WHAT ARE THE CONSEQUENCES OF SHOULDER INSTABILITY
Shoulder dislocations damage the anatomical components ensuring joint stability: ligaments, labrum. Furthermore, fractures of the head of the humerus or the glenoid can occur during dislocations.
These dislocations decrease shoulder stability and increase the risk of relapses. This is known as chronic instability or recurrent dislocation.
WHEN SHOULD YOU CONSULT?
Shoulder instability can be an issue when doing some sports such as swimming, handball or tennis, and dislocations can occur during competitions. Patients who have dislocated their shoulder several times often develop apprehension when cocking their arm; they are very wary of putting their arm up and back in case the shoulder dislocates.
Sometimes, after one or several dislocations, there is no apprehension but the shoulder is painful. This is referred to as a unstable painful shoulder.
When the apprehension or the pain becomes troublesome, it can be useful to consult to assess the damage and look at possible treatments.
WHAT EXAMINATIONS ARE NECESSARY?
The different examinations aim to assess the damage caused by the dislocations and choose the most suitable operation to stabilise the shoulder.
The examinations must include x-rays to see if there are any fractures of the glenoid or the head of the humerus. A MRI arthrogram which is a scan with the injection of an x-ray contrast medium in the shoulder, and a CT scan with 3D reconstruciton is often performed as well to visualise any damage to the labrum.
WHAT IS A CORACOID BLOCK (LATARJET PROCEDURE)?
With recurrent dislocations that disrupt work-life or sports activities, a coracoid block can be proposed. A coracoid block is an operation to stabilise the shoulder in the case of anterior dislocation.
This operation consists in removing part of the coracoid process, a natural bone projection on the shoulder blade located near the glenohumeral joint. This bony projection is cut leaving the conjoint tendon and coracoacromial ligament attached to it. It is then attached using 1 or 2 screws to the front of the glenoid where it should normally fuse.
Stabilisation is achieved thanks to a triple effect. Firstly, it is linked to the transfer of the conjoint tendon, which creates a dynamic sling preventing the head of the humerus from dislocating when the arm is lifted up and back into the position in which the shoulder normally dislocates. Furthermore, the position of the block increases the surface of the glenoid, which also participates in stabilisation. Finally, the joint capsule, which is the envelope around the joint, and the ligaments are tightened and sutured to the coracoacromial ligament still inserted in the coracoid.
Read more about Bone loss in shoulder joint due to Recurrent Dislocation and Latarjet Procedure

The common an highly successful bone augmentation procedure for the shoulder joint is an Open or Arthroscopic Latarjet procedure. The Arthroscopic Latarjet procedure has the advantages of less soft tissue injury, faster rehabilitation and ability to correct other joint problems like SLAP tear or a Remplissage for Hill sach lesion during the procedure.
Watch a video of Arthroscopic Bankart surgery
Case example :
This is a 36year old male patient who presented with recurrent dislocation of the left shoulder joint. He had a rare variant of the Bankart lesion (detachment of the glenoid labrum and capsule from the glenoid bone (cup of the shoulder joint). This is called a Perthe’s lesion where the anterior glenoid labrum has a false attachment to the bone. But this does not have biomechanical strength and the shoulder was weak and unstable on movement. He had a superior labram anterior-posterior tear.
In this video you can see suture anchor fixation of the anteroinferior labrum and the superior labrum.
Patient files
Arthroscopic Latarjet changes life of Violinist

Recent Posts

Sr. Consultant Orthopedic Surgeon, Prof & Head,
Institute of Advanced Orthopedics, MOSC Medical College Hospital, Kolenchery, Kochi, Kerala, India - 682311




