 Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
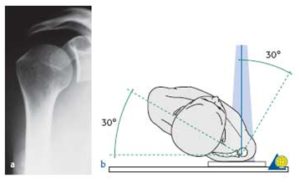
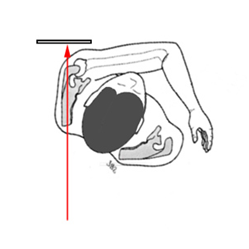
True AP Shoulder (Grashey’s AP)
in neutral rotation
(taken in the plane of the scapula)
Position: Patient erect, turned 30-35° toward the side being xrayed
Tube: Perpendicular to plate
The patient must stand facing the x-ray source with the posterior aspect of the affected side against the x-ray plate. The opposite trunk is rotated at least 30°.
(Grashey view)
- Helpful for:Glenohumeral Arthritis,Coracoid Process Fracture,Glenoid Fracture, Proximal Humerus Fracture. Posterior Glenohumeral Instability.
- Evaluate: humeral head postion relative to glenoid; AC joint position/arthritis; RTC calcifications, acromial spurring
- Acromiohumeral interval: normal = 7-14mm. <7mm indicates Massive RTC Tear. May appear falsely decreased with posterior subluxation of the humeral head.

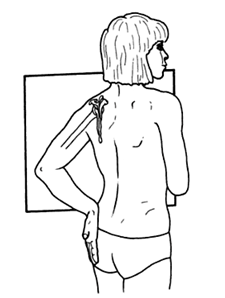
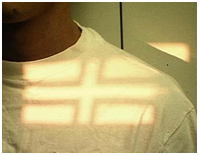
Outlet view Shoulder Xray (Supraspinatus Outlet view)
Position: Erect with anterior aspect of affected shoulder against x-ray plate and rotating other shoulder out 40 deg°.
Beam: aimed from posteriorly along scapular spine but with the beam aimed with 20 ° caudal tilt (10 Deg for scapular Y view)
- Demonstrates: outlet/impingement of the supraspinatus and coracoacromial arch.
- Helpful for:Subacromial Impingement, assessing Subacromial Morphology, unfused acromial epiphysis.


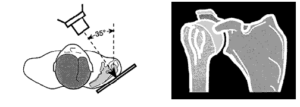
Axillary view Shoulder Xray
Position: Patient seated at side of radiographic table with the arm abducted and axilla over the cassette.
Beam:angle 5°-10° toward the elbow, central beam directed at the shoulder joint.
The patient is supine with the x-ray plate placed above the shoulder. Abduction of about 30º is needed, which can be painful in an acute setting.
Many alternative postions for similar xray, can be supine etc.
- Demonstrates: glenohumeral joint narrowing (best view), Os Acromionale, glenoid version, glenoid erosion, humeral head subluxation.
- Helpful for: determining the amount of acromion which remains in patients who have undergone previous surgery; relation of humeral head to glenoid; Hill-Sachs lesions,Os Acromionale, Acromioclavicular Arthritis, Shoulder Dislocation




Alternative axillary view – A less painful alternative for acute fractures. The patient remains in a comfortable sling and is placed at the edge of the table, a cassette is placed above the shoulder, and the beam is aimed upward from below the table, cranial, through the axilla.
A true axillary view will have an “eye” just posterior to the glenoid
AC joint
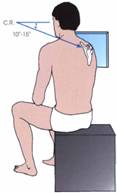
Zanca View Shoulder Xray for AC joint
Position: Erected with cassette behind shoulder.
Beam:Xray beam aimed at the AC joint in 10° to 15° cephalic tilt. Xray penetration should be 1/2 normal to avoid overpenetration of AC joint.
- Demonstrates: AC joint and distal clavicle
- Helpful for:Acromioclavicular Arthritis, Acromioclavicular Joint Separations, Distal Clavicle Osteolysis, Distal Clavicle Fracture
- AC joint spurring and cystic changes indicatesAcromioclavicular Arthritis
- Distal clavicle elevation indicatesAcromioclavicular Joint Separations.


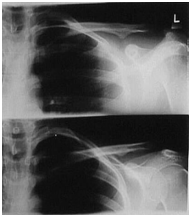
AP Stress view for AC joint
- 10 to 15 pounds Weights in both hands
- Deep Inspiration
Stryker Notch View Shoulder Xray
Position: Patient supine with cassette posterior to the shoulder. The hand placed on top of the head. The elbow should point straight upward.
Beam directed 10° superiorly/toward the head, centered over the coracoid process.
The body is rotated 15 to 45 degrees to get scapula parallel to film
- Demonstrates: humeral head
- Helpful for: Hill-Sachs lesions(best view), Bankart Lesion.



Scapular Y view
PA – placing anterior aspect of affected shoulder against x-ray plate and rotating other shoulder out approximately 40 deg;
– x-ray tube is then placed posteriorly along scapular spine, & this provides a true lateral view of the shoulder




APICAL OBLIQUE VIEW
Indication – Anterior glenoid lip defect
Posterior lateral impression fractures of the humeral head
In this technique the patient sits with the scapula flat against the cassette (as for the AP view in the plane of the scapula). The x-ray beam is centered on the coracoid and directed perpendicular to the cassette (45° to the coronal plane) except that it is angled 45° caudally. The beam passes tangential to the articular surface of the glenohumeral joint and the posterolateral aspect of the humeral head.

Clavicle AP
Centered to clavicle
Suspended Respiration
CLAVICLE PA AXIAL
Horizontal – one inch above center of clavicle. Vertical – centered over clavicle

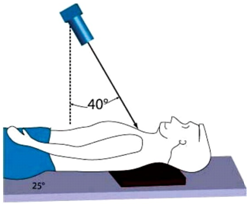
Sternoclavicular joint – SERENDIPITY VIEW
Technique:
– patient is supine;
– non rigid 11 x 14 inch cassette is placed under the upper chest, shoulders, and neck;
– beam is angled 40 deg. cephalad off verticle centered on the sternum;
– tube to cassette distance is 60 deg for adults and 40 deg for child
Arthroscopic Latarjet changes life of Violinist

Recent Posts

Sr. Consultant Orthopedic Surgeon, Prof & Head,
Institute of Advanced Orthopedics, MOSC Medical College Hospital, Kolenchery, Kochi, Kerala, India - 682311




