 Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
Call us:+91-484 2885910 (Reception Orthopedics; 9am to 5pm Mon-Sat), +91-484-2885621 (22,23,24)
Doctor's mobile - +91 9497559755 (whatsApp anytime)
Anterior Cruciate Ligament (ACL) reconstruction is a highly successful surgery, but in some patients the ligament may fail due to reinjury, graft stretching, tunnel problems, or persistent instability of the knee. When this happens, a revision ACL reconstruction may be required to restore stability and allow a safe return to daily activities and sports.
Revision surgery is more complex than the first operation and requires careful planning. Modern techniques allow surgeons to address not only the ligament itself but also other factors that contribute to instability.
Why Do ACL Reconstructions Fail?
Common reasons include:
- Reinjury or high-energy sports trauma
- Improper tunnel placement in the previous surgery
- Weak or stretched graft tissue
- Associated ligament injuries
- Persistent rotational instability of the knee
- Early return to sports before full healing
A detailed evaluation with clinical examination, MRI, and sometimes CT scans helps determine the best revision strategy.
Modern Options in Revision ACL Surgery
Revision ACL reconstruction is no longer just about replacing the ligament. Surgeons now combine several techniques to improve stability and protect the new graft.
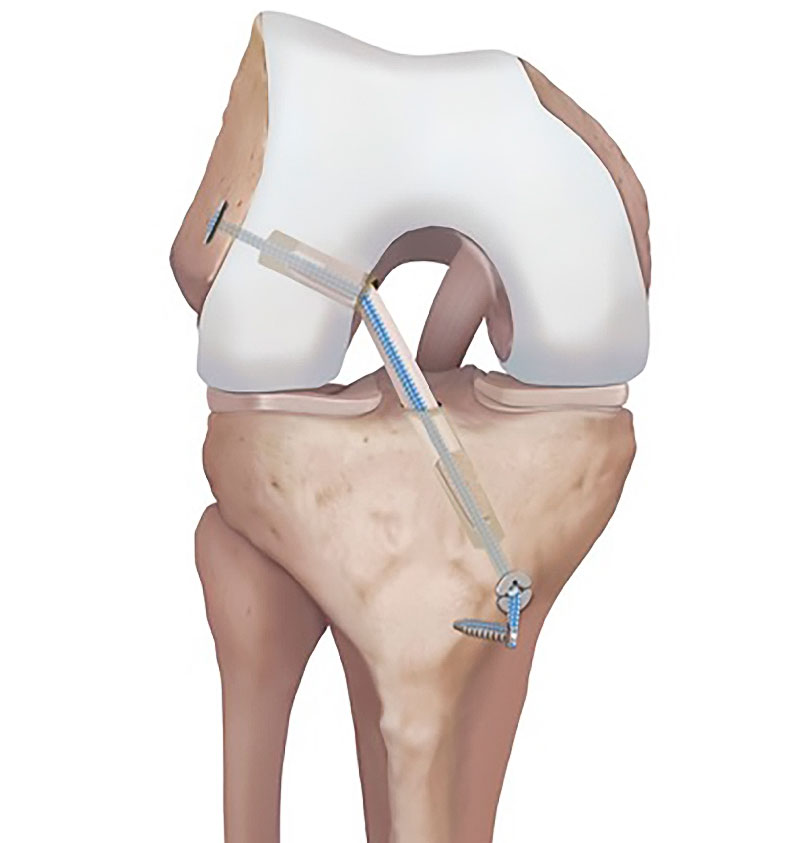
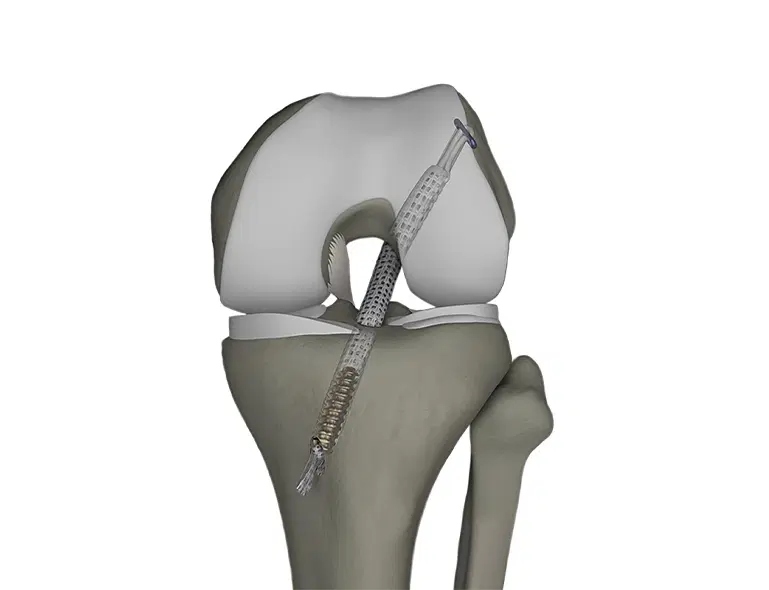
1. Revision ACL Reconstruction
The failed ligament is removed and a new graft is reconstructed using precise tunnel placement and advanced fixation techniques. The goal is to restore the normal anatomy and function of the ACL.
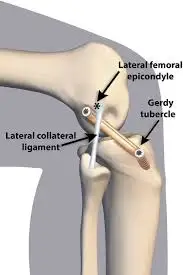
2. Lateral Extra-Articular Tenodesis (LET)
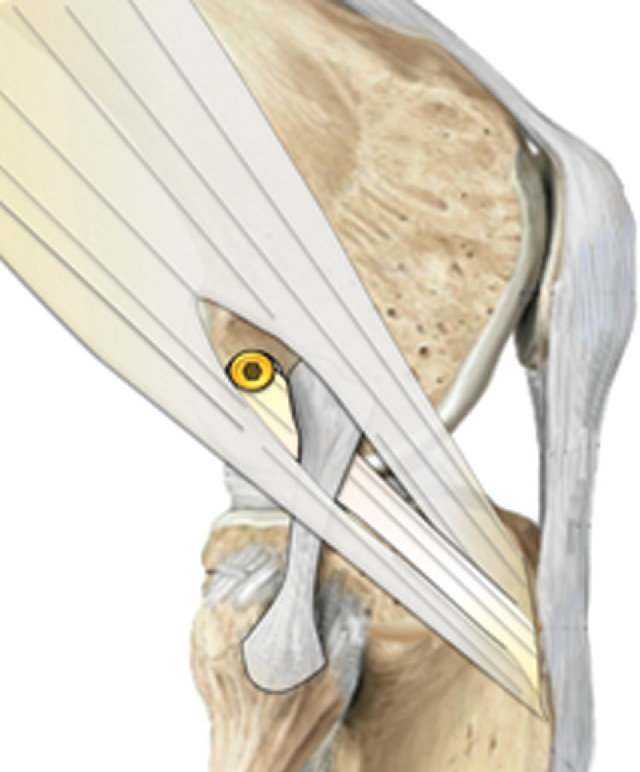
In some patients, particularly those with rotational instability or high-risk sports activity, an additional procedure called lateral extra-articular tenodesis may be performed.
This procedure:
- Reinforces the outer side of the knee
- Controls rotational instability
- Protects the reconstructed ACL graft
- Reduces the risk of re-tear in high-demand athletes
LET is commonly combined with revision ACL surgery in patients who have pivot shift instability or multiple ligament injuries.
3. Internal Bracing
Internal bracing is a modern technique where a strong suture tape is added alongside the reconstructed ligament.
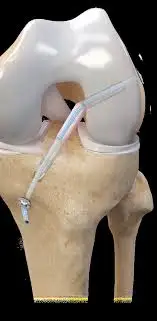
This acts like a seatbelt for the new ACL graft, providing:
- Additional early stability
- Protection during the healing phase
- Reduced stress on the graft during rehabilitation
The internal brace does not replace the ligament but acts as a temporary support while the graft matures.
4. Jewel Augmentation
In cases where the graft may be biologically weaker or when additional support is desirable, Jewel augmentation or mechanical reinforcement techniques may be used.

These methods provide:
- Extra protection for the healing graft
- Improved mechanical strength during early recovery
- Greater confidence during rehabilitation
They are particularly useful in high-risk revision situations. Jewel ACL replacement is a newer technique that uses a high-strength synthetic ligament designed to replicate the function of the native ACL and provide immediate mechanical stability to the knee. Unlike traditional ACL reconstruction that uses tendon grafts, this method relies on a durable implant to restore ligament support. Early studies and clinical experiences have reported promising short-term stability and quicker rehabilitation. However, the available scientific evidence is still limited, and most published results are based on short-term follow-up. Because long-term durability and biological integration are not yet well established, this technique is currently used cautiously and requires further research before it can be widely accepted as a standard replacement for ACL reconstruction.
Choice of Graft in Revision ACL Surgery
Selecting the right graft is a crucial part of revision surgery.
Autograft (Patient’s Own Tissue)
Common autografts include:
- Hamstring tendon
- Peroneus Longus tendon
- Quadriceps tendon
- Patellar tendon
Advantages of Autograft
- Living biological tissue from the patient
- Faster incorporation and healing
- Lower failure rates in young athletes
- No risk of disease transmission
Autografts are often preferred in young, active patients and revision cases.
Allograft (Donor Tissue)
Allografts are grafts obtained from tissue banks.
Advantages of Allograft
- No graft harvest from the patient
- Shorter surgical time
- Less postoperative donor-site pain
However, in young high-demand patients, allografts may have higher re-tear rates, so they are usually reserved for selected situations.
Recovery After Revision ACL Surgery
Recovery after revision surgery is carefully structured and slightly slower than primary ACL reconstruction.
Rehabilitation typically includes:
- Early controlled motion
- Gradual strengthening of muscles
- Progressive return to activities
- Return to sports usually 9–12 months after surgery
Strict adherence to physiotherapy is essential for the best outcome.
Goal of Revision ACL Surgery
The main goals of revision ACL reconstruction are:
- Restore knee stability
- Protect cartilage and meniscus
- Allow safe return to sports and activities
- Reduce the risk of further knee damage
With modern techniques and careful patient selection, revision ACL surgery can achieve excellent stability and long-term knee function.
Arthroscopic Latarjet changes life of Violinist

Recent Posts

Sr. Consultant Orthopedic Surgeon, Prof & Head,
Institute of Advanced Orthopedics, MOSC Medical College Hospital, Kolenchery, Kochi, Kerala, India - 682311




